DMSO Could Save Millions From Brain and Spinal Injury
The decades of evidence showing DMSO revolutionizes the care of many "untreatable" circulatory and neurologic conditions.
DMSO in Context
Because DMSO had the fortune to be discovered at a time when there was still an unbridled enthusiasm within the scientific community to investigate an unorthodox idea (something which has largely disappeared now because career scientists are so dependent upon not rocking the boat to ensure a lifetime supply of research grants) and it fell into the right people’s lap (exceptionally talented, ethical and driven physicians who’d earned the support of their superiors) the scientific community rallied behind it and published thousands of papers on DMSO.
Nonetheless, the FDA was still able to squelch it, and all of the research behind it (along with all the animals that were sacrificed to attain it) have been consigned to the dustbins of history. In the case of DMSO, this is particularly tragic because of how much suffering (and economic cost) many of the disorders discussed here create and the fact that decades of research and billions of research dollars have brought us no closer to solving them.
I thus made the decision to present this in a neutral tone and do my best to accurately present that science behind DMSO (which has required hundreds of hours of work) so I could give DMSO the best chance of flourishing now and helping those it could help—but in truth—words cannot begin to express my disdain over how DMSO was treated or the human cost of the callous bureaucratic dictates which have kept it from being adopted within the medical system (a sentiment I believe will be shared by many of you). For example, this is what Pierre Kory said after I asked him to review this article:
In the over 15 years I spent running ICU’s managing many kinds of brain injuries, strokes and bleeds, it both infuriates and saddens me to know of an intervention that could’ve helped so many of the hundreds of devastating neurological illnesses that I valiantly and often largely unsuccessfully tried to reverse to health. The therapeutic strategies that I had to rely on like tPa were often quite limited in impact or introduced major risks to the patient.
Note: the reason this project has taken so long is because even here, I only touched the tip of the iceberg, and there are still many other paradigm shifting uses for DMSO (e.g., it is a safe and effective painkiller, it treats both acute musculoskeletal injuries and chronic ones creating significant physical impairment, and it provides a way to treat many other challenging conditions that still do not have an effective therapy within the standard of care). In turn my hope is provide the rest of the DMSO in the near future.
As so much has been forgotten about DMSO, few are aware of its intravenous applications (even its proponents). In the final part of this article, I will discuss everything we know on the subject (e.g., where to procure it, what supplies to use, how to dose it) and the non-IV protocols we’ve used for strokes (since IV DMSO was often not feasible in those situations) and other traumatic injuries both at the time of injury and afterward for recovery (e.g., IV DMSO is one of the best options for stroke rehabilitation).
Story at a Glance:
•DMSO is a remarkably safe chemical that protects cells from otherwise fatal stressors (e.g., freezing, burning, shockwaves, ischemia). Since the heart, brain, and spinal cord are particularly vulnerable to injury, DMSO can produce miraculous results for those conditions.
•The usage of DMSO completely transforms the management of strokes (including brain bleeds), heart attacks, and spinal cord injuries. As I will show here, had the FDA not sabotaged DMSO’s adoption, in addition to countless lives being saved, millions could have been protected from a lifetime of disability or paralysis.
•DMSO has many other remarkable properties. For example, it stabilizes proteins, and thus treats many challenging protein disorders (e.g., amyloidosis and numerous genetic disorders).
•Many conditions DMSO treats are typically considered to be incurable. In this article, I will focus on DMSO’s remarkable utility for the conditions that respond best to intravenous DMSO (e.g., a variety of circulatory disorders like varicose veins or Raynaud’s) and complex neurological disorders (e.g., Down Syndrome, Developmental Delay, ALS, Alzheimer’s, Parkinson’s), along with how to administer IV DMSO and DMSO stroke protocols.
If I were stranded on a desert island or knew the world was ending and I could only bring a few therapies with me, one of them, without a doubt, would be DMSO. This is because:
•It treats a wide range of severe illnesses which are often otherwise incurable and frequently fatal or lead to a lifetime of permanent disability.
•It effectively treats acute injuries and rehabilitates chronic musculoskeletal disorders (e.g., arthritis). Because of this, it’s one of the best “pain medicines” out there and has allowed many to get their lives back.
•It has a variety of unique properties that open up a completely different dimension to how medicine can be practiced.
•It is one of the safest medically active substances in existence.
Remarkably, in the 1960s, this was recognized and DMSO took the nation by storm (e.g., people everywhere were clamoring for it, gas stations would often advertise they sold it, and tens of thousands of research studies were conducted by enthusiastic scientists around the globe). Now however, outside of it being a laboratory chemical or an alternative therapy some people use for joint pain, few are even aware of DMSO’s existence.
This was due to the FDA waging a multi-decade long war against DMSO (despite widespread outcry from Congress and the public), which I believe was arguably the worst thing the FDA has ever done to the country.
Since I am uniquely positioned to present many of the forgotten sides of medicine to the public, I’ve long felt the DMSO story needs to be told. Simultaneously however, since there is a wealth of data on this topic, I wanted to ensure I honored the importance of this subject and accurately present it. For this reason, I’ve spent the last three months reading and arranging thousands of pages of literature. Since there is so much to say on this topic, this series will be broken into a few parts. In the first installment, I will cover the key properties of DMSO and the challenging conditions where it provides the most profound benefits.
What is DMSO?
Dimethyl sulfoxide, as the name implies, is comprised of two methyl groups and an oxygen atom bonded to sulfur. This simple chemical and its breakdown products exist in nature (e.g., they can be found in small amounts in milk, tomatoes, tea, coffee, beer clams, and cooked corn, while the salty smell of the ocean is, in part, due to microalgae near the surface creating dimethyl sulfoxide—some of which also makes it into the rain).
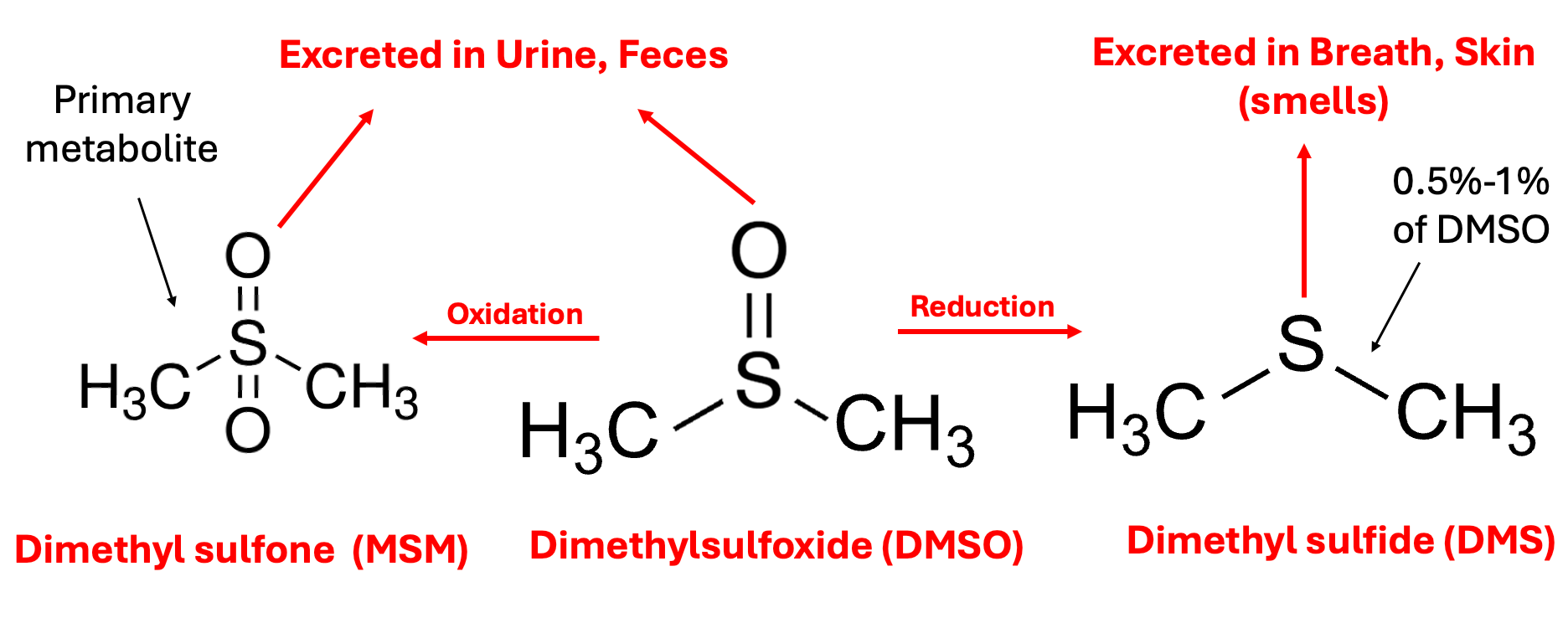
In the body, DMSO is then oxidized or reduced, with the oxidized form (more commonly known by the name methylsulfonylmethanethe or MSM—a common joint healing supplement) being the primary fate of it, while the reduced form DMS (which naturally exists in trace amounts in the body) is the more notorious metabolite because it is responsible for DMSO’s characteristic “side effect,” a distinctive garlic or clam-like odor (or taste) that is excreted through the mouth and skin which certain individuals have difficulty tolerating (and forcing certain longterm DMSO users to creatively arrange their social life). This effect typically lasts a few hours, but in certain cases can last up to 72 hours, and appears to be reflective of the overall health of the body (since as people detox, their DMSO odor decreases).
Note: one school of thought in integrative medicine (e.g., Dr. Mercola is a strong proponent of this model) argues that insufficient oxidation, which leads to a build-up of reduced molecules in the body (termed reductive stress) is a root cause of many illnesses (e.g., the mitochondria cannot function properly if the electron transport chain is reduced). The susceptibility to the DMSO odor is one of the best illustrations I have found of this model, particularly since there are many reports showing that concurrently taking chlorine dioxide (an oxidizing agent) eliminates it (as does a user’s overall health improving over time). Likewise, some DMSO users and one study have found that when DMSO was taken at the same time as alcohol (another oxidizing agent), the odor was reduced, whereas when alcohol was given an hour after DMSO, the opposite occurred (which touches upon the fact DMSO can sometimes cause excessive drowsiness if combined with a sedative).
Due to its relatively small size, having both a polar and non-polar half, being able to form hydrogen bonds slightly stronger than those found between water molecules, and not releasing protons, DMSO has two remarkable properties:
•It acts as a near-universal solvent (e.g., it interacts with a vast range of biomolecules and can easily mix with any concentration of water).
•It’s able to pass through biological membranes without damaging them (something to my knowledge, nothing else can do).
Because of this, DMSO will rapidly enter the body (including the brain) regardless of its route of administration (e.g., within 5 minutes after going on the skin it can be found in the blood, and within an hour it can be found within the bones), but simultaneously does not accumulate within the body after prolonged use (and virtually none remains a week after administration).
Note: in one study of rats, radio-labeled DMSO was found to enter all tissues of the body within 30 minutes (with the highest levels seen in the plasma, kidney, spleen, lung, heart, and testes and the lowest in the lens of the eye), with DMSO levels declining to minimal levels after 24 hours, another study found over 90% of topically applied DMSO is absorbed with tissue concentrations peaking 1.5 to 2 hours after topical administration (and 85% being excreted unchanged in the urine after 24 hours) while another study found orally administered DMSO reached a peak blood level in 4 hours and was undetectable after 120 hours, while MSM appeared in the blood after 48 hours and disappeared after 400 hours (with another human study finding similar results).
DMSO in turn, has an almost endless amount of uses as it can be applied in almost any manner (e.g., it is frequently applied through the skin—although less is absorbed in this manner than the other routes of administration). Almost any drug or substance can be combined with it and administered through the skin (e.g., steroids, NSAIDs, numerous antibiotics or antivirals, glucose, vitamin C, hydrogen peroxide, or chlorine dioxide). In many cases, the effect of those drugs is enhanced, and simultaneously, their toxicity is reduced (although, in some cases, the toxicity increases).
Note: DMSO is less effective at bringing larger molecules into the body (e.g., it had been hoped it could be mixed with insulin so diabetics could have a way to bypass the need for injecting insulin—but this didn’t work).
The article has further sections with the following subtitles:
Cellular Protection
Circulatory Disorders
Heart Attacks
Current Stroke Management
Ischemic Strokes
Hemorrhagic Strokes and Traumatic Brain Injuries
Spinal Cord Injuries
DMSO and Protein Folding
Cognitive Impairment and Dementia
Psychiatric Conditions
Developmental Disabilities
Article Link: https://www.midwesterndoctor.com/p/dmso-could-save-millions-from-brain


This Forum message belongs to a larger discussion thread. See the complete thread below. You can reply to this message!
-
DMSO Could Save Millions From Brain and Spinal Inj...
 turiya
4 d
68
turiya
4 d
68
This is the position of the above message within the thread.
CureZone Newsletter is distributed in partnership with https://www.netatlantic.com
Contact Us - Advertise - Stats
0.047 sec, (9)