
(FIGURE 8.5. Minnesota volunteers at mealtime. Copyright 1950 by the University of Minnesota Press. Reprinted by permission)
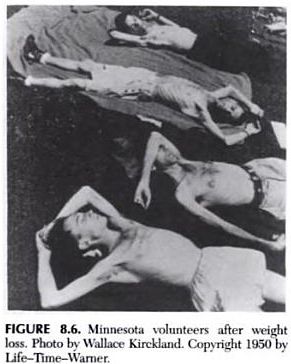
(FIGURE 8.6. Minnesota volunteers after weight loss. Photo by Wallace Kirkland. Copyright 1950 by Life-Time-Warner.)
Human Experiment: The Effects of Starvation on Behavior by mouseclick ..... Fasting: Water Only
Date: 6/2/2009 8:09:49 AM ( 15 y ago)
Hits: 60,786
URL: https://www.curezone.org/forums/fm.asp?i=1430817
1 of 1 (100%) readers agree with this message. Hide votes What is this?
One of the roast important advancements in the understanding of eating disorders is the recognition that severe and prolonged dietary restriction can lead to serious physical and psychological complications. Many of the symptoms once thought to be primary features of anorexia nervosa are actually symptoms of starvation.
Given what we know about the biology of weight regulation, what is the impact of weight suppression on the individual? This is particularly relevant for those with anorexia nervosa, but is also important for people with eating disorders who have lost significant amounts of body weight. Perhaps the most powerful illustration of the effects of restrictive dieting and weight loss on behavior is an experimental study conducted almost 50 years ago and published in 1950 by Ancel Keys and his colleagues at the University of Minnesota (Keys et al., 1950). The experiment involved carefully studying 36 young, healthy, psychologically normal men while restricting their caloric intake for 6 months. More than 100 men volunteered for the study as an alternative to military service; the 36 selected had the highest levels of physical and psychological health, as well as the most commitment to the objectives of the experiment.
During the first 3 months of the experiment, the volunteers ate normally while their behavior, personality, and eating patterns were studied in detail. During the next 6 months, the men were restricted to approximately half of their former food intake and lost, on average, approximately 25% of their former weight. Figure 8.5 shows the Minnesota volunteers at mealtime, and Figure 8.6 reveals the physical results of the weight loss. Although this was described as a study of semistarvation, it is important to keep in mind that cutting the mens rations to half of their former intake is precisely the level of caloric deficit used to define conservative treatments for obesity (Stunkard, 1987). The 6 months of weight loss were followed by 3 months of rehabilitation, during which the men were gradually refed. A subgroup was followed for almost 9 months after the refeeding began. Most of the results were reported for only 32 men, since 4 men were withdrawn either during or at the end of the semistarvation phase. Although the individual responses to weight loss varied considerably, the men experienced dramatic physical, psychological, and social changes. In most cases, these changes persisted during the rehabilitation or renourishment phase.
What makes the starvation study (as it is commonly known) so important is that many of the experiences observed in the volunteers are the same as those experienced by patients with eating disorders. This section of this chapter is a summary of the changes observed in the Minnesota study. All quotations followed by page numbers in parentheses are from the original report by Keys et al. (1950) and are used by permission of the University of Minnesota Press.
(FIGURE 8.5. Minnesota volunteers at mealtime. Copyright 1950 by the University of Minnesota Press. Reprinted by permission)
(FIGURE 8.6. Minnesota volunteers after weight loss. Photo by Wallace Kirkland. Copyright 1950 by Life-Time-Warner.)
One of the most striking changes that occurred in the volunteers was a dramatic increase in food preoccupations. The men found concentration on their usual activities increasingly difficult, because they became plagued by incessant thoughts of food and eating. Figure 8.7 illustrates the increase in the average ratings of concern about food, as well as corresponding declines in interest in sex and activity, for 32 subjects at different stages of semistarvation and rehabilitation. Food became a principal topic of conversation, reading, and daydreams.
As starvation progressed, the number of men who toyed with their food increased. They made what under normal conditions would be weird and distasteful concoctions. (p. 832) . . . Those who ate in the common dining room smuggled out hits of food and consumed them on their bunks in a long-drawn-out ritual. (p. 833). Cookbooks, menus, and information bulletins on food production became intensely interesting to many of the men who previously had little or no interest in dietetics or agriculture. (p. 833) . . . [The volunteers] often reported that they got a vivid vicarious pleasure from watching other persons eating from just smelling food. (p. 834)
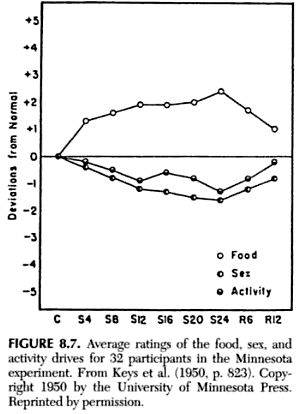
(FIGURE 8.7. Average ratings of the food, sex, and activity drives for 32 participants in the Minnesota experiment. From Keys et al. (1950, p. 823). Copyright 1950 by the University of Minnesota Press. Reprinted by permission)
In addition to cookbooks and collecting recipes, some of the men even began collecting coffeepots, hot plates, and other kitchen utensils. According to the original report, hoarding even extended to non-food-related items, such as: old books, unnecessary second-hand clothes, knick knacks, and other junk. Often after making such purchases, which could be afforded only with sacrifice, the men would he puzzled as to why they had bought such more or less useless articles (p. 837). One man even began rummaging through garbage cans. This general tendency to hoard has been observed in starved anorexic patients (Crisp, Hsu, & Harding, 1980) and even in rats deprived of food (Fantino & Cabanac, 1980). Despite little interest in culinary matters prior to the experiment, almost 40% of the men mentioned cooking as part of their postexperiment plans. For some, the fascination was so great that they actually changed occupations after the experiment; three became chefs, and one went into agriculture!
During semistarvation, the volunteers eating habits underwent remarkable changes. The men spent much of the day planning how they would eat their allotment (If food. Much of their behavior served the purpose (If prolonging ingestion and increasing the appeal or salience of food. The men often ate in silence and devoted total attention to food consumption.
The Minnesota subjects were often caught between conflicting desires to gulp their food down ravenously and consume it slowly so that the taste and odor of each morsel would be fully appreciated. Toward the end of starvation some of the men would dawdle for almost two hours over a meal which previously they would have consumed in a matter of minutes.. . . They did much planning as to how they would handle their days allotment of food. (p. 833)The men demanded that their food be served hot, and they made unusual concoctions by mixing foods together, as noted above. There was also a marked increase in the use of salt and spices. The consumption of coffee and tea increased so dramatically that the men had to be limited to 9 cups per day; similarly, gum chewing became excessive and had to be limited after it was discovered that one man was chewing as many as 40 packages of gum a day and developed a sore mouth from such continuous exercise (p. 835).
During the 12-week refeeding phase of the experiment, most of the abnormal attitudes and behaviors in regard to food persisted. A small number of men found that their difficulties in this area were quite severe during the first 6 weeks of refeeding:
In many cases the men were not content to eat normal menus but persevered in their habits of making fantastic concoctions and combinations. The free choice of ingredients, moreover, stimulated creative and experimental playing with food . . . licking of plates and neglect of table manners persisted. (p. 843)
During the restrictive dieting phase of the experiment, all of the volunteers reported increased hunger. Some appeared able to tolerate the experience fairly well, but for others it created intense concern and led to a complete breakdown in control. Several men were unable to adhere to their diets and reported episodes of binge eating followed by self-reproach. During the eighth week of starvation, one volunteer flagrantly broke the dietary rules, eating several sundaes and malted milks; he even stole some penny candies. He promptly confessed the whole episode, [and] became self-deprecatory (p. 884). While working in a grocery store, another man suffered a complete loss of will power and ate several cookies, a sack of popcorn, and two overripe bananas before he could regain control of himself. He immediately suffered a severe emotional upset, with nausea, and upon returning to the laboratory he vomited. ... He was self-deprecatory, expressing disgust and self-criticism. (p. 887)
One man was released from the experiment at the end of the semistarvation period because of suspicions that he was unable to adhere to the diet. He experienced serious difficulties when confronted with unlimited access to food: He repeatedly went through the cycle of eating tremendous quantities of food, becoming sick, and then starting all over again (p. 890).
During the refeeding phase of the experiment, many of the men lost control of their appetites and ate more or less continuously (p. 843). Even after 12 weeks of refeeding, the men frequently complained of increased hunger immediately following a large meal:
[One of the volunteers] ate immense meals (a daily estimate of 5,0006,000 cal.) and yet started snacking an hour after he finished a meal. [Another] ate as much as he could hold during the three regular meals and ate snacks in the morning, afternoon and evening. (p. 846)
Such overeating took its toll:
This gluttony resulted in a high incidence of headaches, gastrointestinal distress and unusual sleepiness. Several men had spells of nausea and vomiting. One man required aspiration and hospitalization for several (lays. (p. 843)
During the weekends in particular, some of the men found it difficult to stop eating. Their daily intake commonly ranged between 8,000 and 10,000 calories, and their eating patterns were described as follows:
Subject No. 20 stuffs himself until he is bursting at the seams, to the point of being nearly sick and still feels hungry; No. 120 reported that he had to discipline himself to keep from eating so much as to become ill; No. I ate until he was uncomfortably full; arid subject No. 30 had so little control over the mechanics of piling it in that he simply had to stay away from food because he could not find a point of satiation even when he was full to the gills. I ate practically all weekend, reported subject No. 26.... Subject No. 26 would just as soon have eaten six meals instead of three. (p. 847)
After about 5 months of refeeding, the majority of the men reported some normalization of their eating patterns, but for some the extreme overconsumption persisted: No. 108 would eat and eat until he could hardly swallow any more and then he felt like eating half an hour later (p. 847). More than 8 months after renourishment began, most men had returned to normal eating patterns; however, a few were still eating abnormal amounts: No. 9 ate about 25 percent more than his pre-starvation amount; once he started to reduce but got so hungry he could not stand it (p. 847). Factors distinguishing men who rapidly normalized their eating from those who continued to eat prodigious amounts were not identified. Nevertheless, the main findings here are as follows: Serious binge eating developed in a subgroup of men, and this tendency persisted in some cases for months after free access to food was reintroduced; however, the majority of men reported gradually returning to eating normal amounts of food after about 5 months of refeeding. Thus, the fact that binge eating was experimentally produced in some of these normal young men should temper speculations about primary psychological disturbances as the cause of hinge eating in patients with eating disorders. These findings are supported by a large body of research indicating that habitual dieters display marked overcompensation in eating behavior that is similar to the binge eating observed in eating disorders (Polivy & Herman, 1985, 1987; Wardle & Beinart, 1981).
The experimental procedures involved selecting volunteers who were the most physically and psychologically robust: The psychobiological stamina of the subjects was unquestionably superior to that likely to be found in any random or more generally representative sample of the population (pp. 915-916). Although the subjects were psychologically healthy prior to the experiment, most experienced significant emotional deterioration as a result of semistarvation. Most of the subjects experienced periods during which their emotional distress was quite severe; almost 20% experienced extreme emotional deterioration that markedly interfered with their functioning.
Depression became more severe during the course of the experiment. Elation was observed occasionally, but this was inevitably followed by low periods. Mood swings were extreme for some of the volunteers:
[One subject] experienced a number of periods in which his spirits were definitely high These elated periods alternated with times in which he suffered a deep dark depression. [He] felt that he had reached the end of his rope [and] expression the fear that he was going crazy.. . [and] losing his inhibitions. (p. 903)
Irritability and frequent outbursts of anger were common, although the men had quite tolerant dispositions prior to starvation. For most subjects, anxiety became more evident. As the experiment progressed, many of the formerly even-tempered men began biting their nails or smoking because they felt nervous. Apathy also became common, and some men who had been quite fastidious neglected various aspects of personal hygiene.
During semistarvation, two subjects developed disturbances of psychotic proportions. One of these was unable to adhere to the diet and developed alarming symptoms:
[He exhibited] a compulsive attraction to refuse amid a strong, almost compelling, desire to root in garbage cans [for food to eat]. He became emotionally disturbed enough to seek admission voluntarily to the psychiatric ward of the University Hospitals. (p. 890)
After 9 weeks of starvation, another subject also exhibited serious signs of disturbance:
[He went on a] spree of shoplifting, stealing trinkets that had little or no intrinsic value. . . . He developed a violent emotional outburst with flight of ideas, weeping, talk of suicide and threats of violence. Because of the alarming nature of his symptoms, he was released from the experiment and admitted to the psychiatric ward of the University Hospitals. (p. 885)
During the refeeding period, emotional disturbance (lid not vanish immediately hut persisted for several weeks, with some men actually becoming more depressed, irritable, argumentative, and negativistic than they had been during semistarvation. After two weeks of refeeding, one man reported his extreme reaction in his diary:
I have been more depressed than ever in my life . I thought that there was only one thing that would pull me out of the doldrums, that is release from C.P.S. [the experiment] I decided to get rid of some fingers. Ten days ago, I jacked up my car and let the car fall on these fingers . It was premeditated. (pp. 894-895)
Several days later, this man actually did chop off three fingers of one hand in response to the stress.
Standardized personality testing with the Minnesota Multiphasic Personality Inventory (MMPI) revealed that semistarvation resulted in significant increases on the Depression, Hysteria, and Hypochondriasis scales. This profile has been referred to as the neurotic triad and is observed among different groups of disturbed individuals (Greene, 1980). The MMPJ profiles for a small minority of subjects confirmed the clinical impression of incredible deterioration as a result of semistarvation. Figure 8.8 illustrates one mans personality profile: Initially it was well within normal limits, but after 10 weeks of semistarvation and a weight loss of only about 4.5 kg (10 pounds, or approximately 7% of his original body weight), gross personality disturbances were evident. On the second testing, all of the MMPI scales were elevated, indicating severe personality disturbance on scales reflecting neurotic as well as psychotic traits. Depression and general disorganization were particularly striking consequences of starvation for several of the men who became the most emotionally disturbed.
The extraordinary impact of scm istarvation was reflected in the social changes experienced by most of the volunteers. Although originally quite gregarious, the men became progressively more withdrawn and isolated. Humor and the sense of comradeship diminished amidst growing feelings of social inadequacy:
Social initiative especially and sociability in general, underwent a remarkable change. The men became reluctant to plan activities, to make decisions, and to participate in group activities.... They spent more and more time alone. It became too much trouble or too tiling to have contact with other people. (pp. 836-837)
The volunteers social contacts with women also declined sharply during semistarvation. Those who continued to see women socially found that the relationships became strained. These changes are illustrated in the account from one mans diary:
I am one of about three or four who still go out with girls. I fell in love with a girl during the control period but I see her only occasionally noxv. Its almost too much trouble to see her even when she visits me in the lab. It requires effort to hold her hand. Entertainment must be tame. If we see a show, the most interesting part of it is contained in scenes where people are eating. (p. 853)

(FIGURE 8.8. Minnesota Multiphasic Personality Inventory (MMPI) scores for one participant in the Minnesota experiment during the control period (C), and after 10 weeks of calorie restriction (S10) and weight loss of about 7% of his control weight. T scores between 30 and 70 are in the normal range. Hs, Hypochondriasis; D, Depression; Hy, Hysteria; Pd, Psychopathic Deviate; Mf, Masculinity-Femininity; Pa, Paranoia; Pt, Psychasthenia; Sc, Schizophrenia; Ma, Hypomania. From Keys et al. (1950, p. 856). Copyright 1950 by the University of Minnesota Press. Reprinted by permission)
Sexual interests were likewise drastically reduced (see Figure 8.7). self-gratification, sexual fantasies, and sexual impulses either ceased or became much less common. One subject graphically stated that he had no more sexual feeling than a sick oyster. (Even this peculiar metaphor made reference to food.) Keys et al. observed that many of the men welcomed the freedom from sexual tensions and frustrations normally present in young adult men (p. 840). The fact that starvation perceptibly altered sexual urges and associated conflicts is of particular interest, since it has been hypothesized that this process is the driving force behind the dieting of many anorexia nervosa patients. According to Crisp (1980), anorexia nervosa is an adaptive disorder in the sense that it curtails sexual concerns for which the adolescent feels unprepared.
During rehabilitation, sexual interest was slow to return. Even after 3 months, the men judged themselves to be far from normal in this area. However, after 8 months of re-nourishment, virtually all of the men had recovered their interest in sex.
The volunteers reported impaired concentration, alertness, comprehension, and judgment during semistarvation; however, formal intellectual testing revealed no signs of diminished intellectual abilities.
As the 6 months of semistarvation progressed, the volunteers exhibited man) physical changes, including gastrointestinal discomfort; decreased need for sleep; dizziness; headaches; hypersensitivity to noise and light; reduced strength; poor motor control; edema (an excess of fluid causing swelling); hair loss; decreased tolerance for cold temperatures (cold hands and feet); visual disturbances (i.e., inability to focus, eye aches, spots in the visual fields); auditory disturbances (i.e., ringing noise in the ears); and paresthesias (i.e., abnormal tingling or prickling sensations, especially in the hands or feet).
Various changes reflected an overall slowing of the bodys physiological processes. There were decreases in body temperature, heart rate, and respiration, as well as in basal metabolic rate (BMR). BMR is the amount of energy (in calories) that the body requires at rest (i.e., no physical activity) in order to carry out normal physiological processes. It accounts for about two-thirds of the bodys total energy needs, with the remainder being used during physical activity. At the end of semistarvation, the mens BMRs had dropped by about 40% from normal levels. This drop, as well as other physical changes, reflects the bodys extraordinary ability to adapt to low caloric intake by reducing its need for energy. As one volunteer described it, he felt as if his body flame [were] burning as low as possible to conserve precious fuel and still maintain life process (p. 852). Recent research has shown that metabolic rate is markedly reduced even among dieters who do not have a history of dramatic weight loss (Platte, Wurrnser, Wade, Mecheril, & Pirke, 1996). During refeeding, Keys et al. found that metabolism speeded up, with those consuming the greatest number of calories experiencing the largest rise in BMR. The group of volunteers who received a relatively small increment in calories during refeeding (400 calories more than during semistarvation) had no rise in BMR for the first 3 weeks. Consuming larger amounts of food caused a sharp increase in the energy burned through metabolic processes.
The changes in body fat and muscle in relation to overall body weight during semistarvation and refeeding are of considerable interest (Figure 8.9). While weight declined about 25%, the percentage of body hit fell almost 70%, and muscle decreased about 40%. Upon refeeding, a greater proportion of the new weight was fat; in tile eighth month of rehabilitation, the volunteers were at about 110% of their original body weight hut had approximately 140% of their original body fat!
How did the men feel about their weight gain during rehabilitation? Those subjects who gained the most weight became concerned about their increased sluggishness, general flabbiness, and the tendency of fat to accumulate in the abdomen and buttocks (p. 828). These complaints are similar to those of many eating disorder patients as they gain weight. Besides their typical fear of weight gain, they often report feeling fat and are worried about acquiring distended stomachs. However, as indicated in Figure 8.9, the body weight and relative body fat of the Minnesota volunteers was at the preexperiment levels after about 9 months of rehabilitation
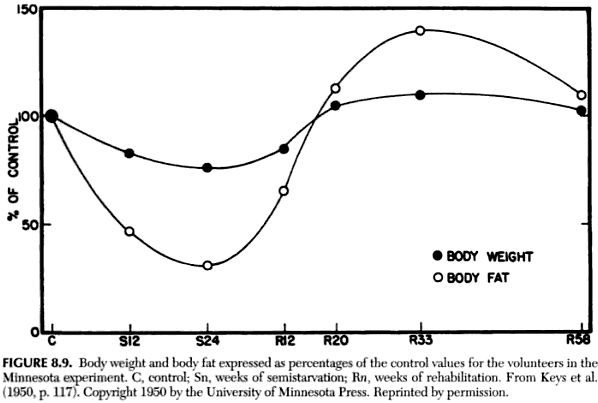
(FIGURE 8.9. Body weight and body fat expressed as percentages of the control values for the volunteers in the Minnesota experiment. C, control; Sn, weeks of semistarvation; Rn, weeks of rehabilitation. From Keys et al. (1950, p. 117). Copyright 1950 by the University of Minnesota Press. Reprinted by permission)
In general, the men responded to semistarvation with reduced physical activity. They became tired, weak, listless, and apathetic, and complained of lack of energy. Voluntary movements became noticeably slower. However, according to Keyes et al., some men exercised deliberately at times. Some of them attempted to lose weight by driving themselves through periods of excessive expenditure of energy in order either to obtain increased bread rations ... or to avoid reduction in rations (p. 828). This is similar to the practice of some eating disorder patients, who feel that if they exercise strenuously, they can allow themselves a bit more to eat. The difference is that for those with eating disorders, the caloric limitations are self-imposed.
As is readily apparent from the preceding description of the Minnesota experiment, many of the symptoms that might have been thought to he specific to anorexia nervosa and bulimia nervosa are actually the results of starvation (Pirke & Ploog, 1987). These are not limited to food and weight, but extend to virtually all areas of psychological and social functioning. Since many of the symptoms that have been postulated to cause these disorders may actually result from undernutrition, it is absolutely essential that weight be returned to normal levels so that psychological functioning can be accurately assessed.
The profound effects of starvation also illustrate the tremendous adaptive capacity of the human body and the intense biological pressure on the organism to maintain a relatively consistent body weight. This makes complete evolutionary sense. Over hundreds of thousands of years of human evolution, a major threat to the survival of the organism was starvation. If weight had riot been carefully modulated and controlled internally, early humans most certainly would simply have died when food was scarce or when their interest was captured by countless other aspects of living. The Keys et al. starvation study illustrates how the human being becomes more oriented toward food when starved and how other pursuits important to the survival of the species (e.g., social and sexual functioning) become subordinate to the primary drive toward food.
One of the most notable implications of the Minnesota experiment is that it challenges the popular notion that body weight is easily altered if one simply exercises a bit of willpower. It also demonstrates that the body is not simply reprogrammed at a lower set point once weight loss has been achieved. The volunteers experimental diet was unsuccessful in overriding their bodies strong propensity to defend a particular weight level. Again, it is important to emphasize that following the months of refeeding, the Minnesota volunteers did not skyrocket into obesity. On the average, they gained hack their original weight plus about 10%; then, over the next 6 months, their weight gradually declined. By the end of the follow-up period, they were approaching their preexperiment weight levels.
Sources: Handbook of Treatments for Eating Disorders - page 153 - 161 (Free on Google Books)
For information. Please note:
<< Return to the standard message view
fetched in 0.02 sec, referred by http://www.curezone.org/forums/fmp.asp?i=1430817